
The Asylum
How our modern psych ward came to be.
People are always shocked when I tell them: the modern psychiatric ward you see today? A direct descendent of an asylum. The folks that you consult with on your DTC pharmacy app that delivers prescriptions to your front door? 100 years ago, they would've been in those wards, administering what they thought was the best care for the mentally ill.
Today we'll be taking a quick look at how care for the mentally ill transformed from madhouses to asylum institutions to community health centers. I'll be dropping some grisly photos — so considered yourself warned!
Before Asylums
Wherever you have humans, you have mental disorders. Lunatics, madmen, the feebleminded, the "crazy" uncle you lock away in the attic — the words have changed but the illness remains the same.
Before the 1700s, if you were mentally ill, you were most likely cared for (or locked up) by your family members. Our understanding of mental illness at this time was vastly limited to 1) demonic possession or 2) a moral/spiritual failing. Families who dealt with mental illness often dealt with it shamefully in their homes, attributing the presence of these illnesses as a ‘punishment’ for something they had done.
When the mentally ill could no longer be supported by their families, they were sent to one of the following:
Almshouses/community housing
These were charitable housing provided for the elderly or disabled in the community, usually funded by the community, the royalty, or the local church. Don't let the word “charitable” trick you — they were terrible places to live, and as a bonus, the mentally ill were often chained to walls and isolated.Workhouses/Poorhouses
Like an almshouse, except you get to work to "earn your keep". Built to keep the poor off the streets, these houses were always underfunded and overpopulated.Prisons
No explanation needed.
The birth of the asylum
In the late 1700s, Englishman William Tuke introduced a new way to provide care — the “moral treatment".
This treatment was based on the assumption that if the mentally ill were treated regularly and encouraged to behave rationally, they could be cured. Tuke housed his patients in serene, rural settings, gave his patients privileges, and provided meaningful work and recreation opportunities. Patients operated under a system where rational behaviors were rewarded, and physical restraints were sparingly used. This "moral treatment" exploded in popularity, and the mental health institution, aka the asylum, was born.
It took a couple of decades for the asylum to make its way to the States, and it wasn't until 1845 that the first asylum was approved of in New Jersey. This was largely credited to Dorothea Dix, an activist who testified against the horrendous treatment of the mentally ill and continuously pushed for mental health reform across state lines. Dorothea played a role in the creation of more than 30 asylums in the States, and by 1965, there were almost 100.
The design of the asylum
I think an incredibly fascinating part of the “mass asylum production” story relates to how they were designed.
Most of the new asylums were built under the "Kirkbride Plan", a building design created by a psychiatrist Thomas Kirkbride. I'm not quite sure how a psychiatrist managed to level up and design a goddamn mental institution, because these asylums weren‘t just a house on a lot.
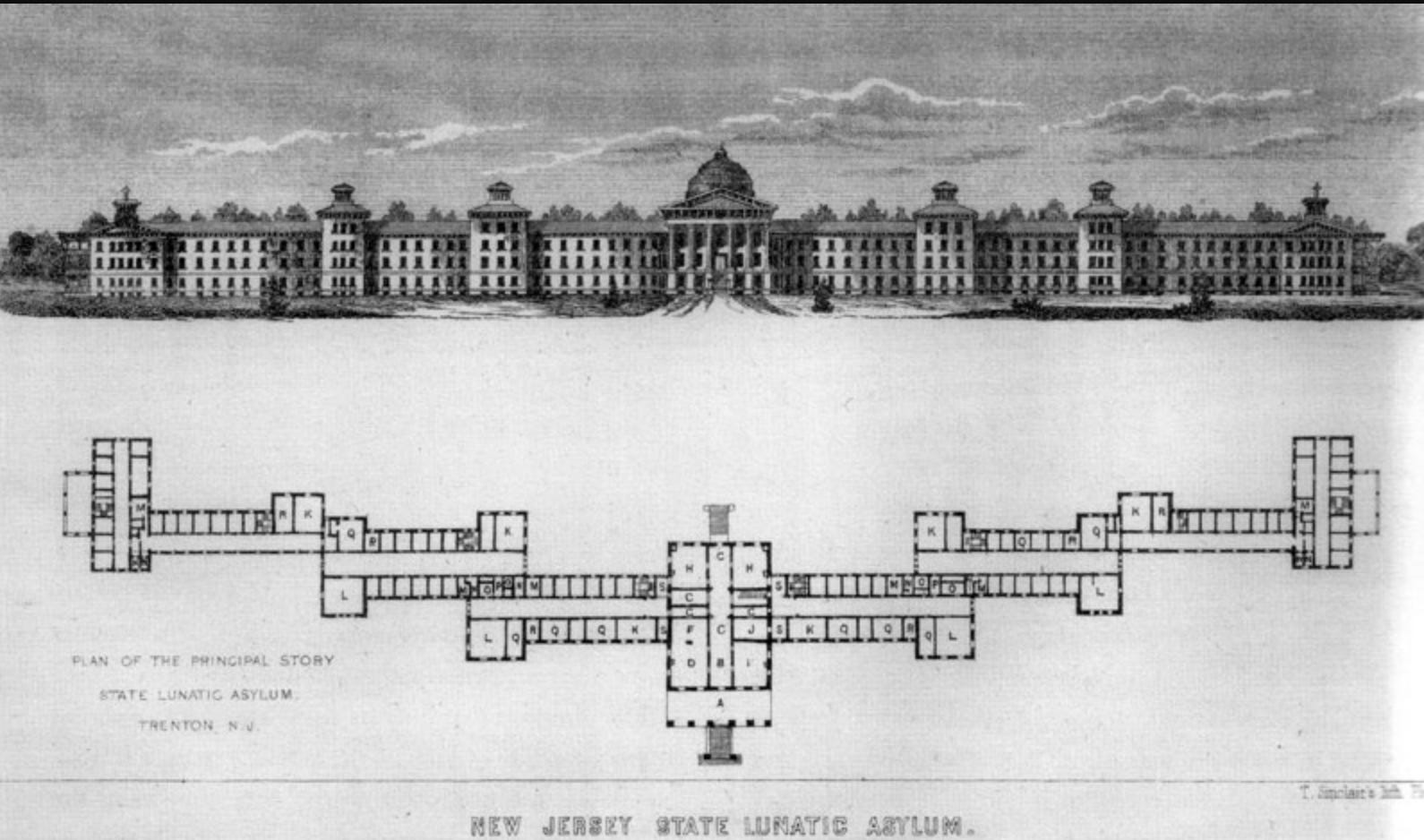
Caption: The first asylum built under the Kirkbride plan, in 1848.
Kirkbride created winged buildings that staggered, allowing each corridor to receive sunlight and air ventilation, which he believed would aid the patients’ healing. Building fronts were grandiose and imposing, and the single-occupancy rooms were spacious with high ceilings. Kirkbride also thought through where everyone lived: admin and “calmer” patients lived in the middle of the wings, while volatile patients lived at the ends.
I also found his plan to be incredibly progressive — Kirkbride suggested equal gender distribution amongst the staff, and also proposed liberal compensation for employees. He provided housing as needed and brought in carpenters, cooks, gardeners, seamstresses, launderers, and even a carriage driver. In short, the Kirkbride asylum was the original Google campus.
The Downfall of the Asylum
As the number of asylums grew from the 1850s to the 1950s, so did the number of patients. Folks lived longer, populations increased, and soon the demand for stays at these asylums outweighed their ability to provide care. Officials of counties also saw the state-run asylums as a financial opportunity — if they transferred their patients to the asylums, they would save some money.
By the 1950s, it's estimated that half a million Americas were in these asylums, living in overcrowded, poor conditions. It also didn't help that the States was coming out of two World Wars and a Great Depression — forcing cuts in both budget and staff.
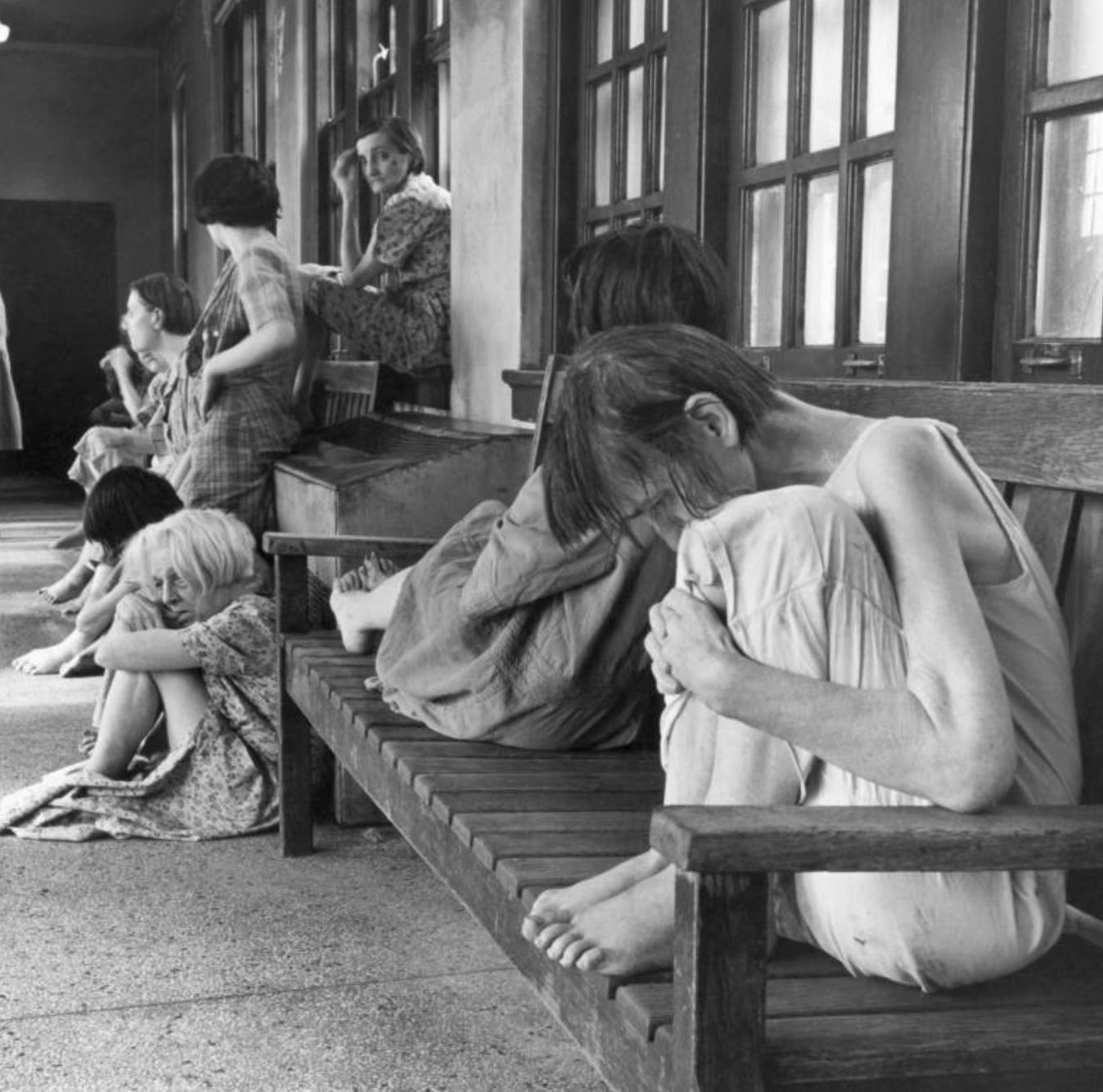
Caption: Patients sit inside Ohio's Cleveland State Mental Hospital in 1946.
Credits: Mary Delaney Cooke/Corbis via Getty Images
I think one important thing to remember is: these state-run asylums were crucial to the field of psychiatry, providing (for better or worse) places of practice throughout the world. We can criticize the use of inhumane techniques like lobotomies, shock therapies, and harsh restraints while also acknowledging that those techniques were the medical standard at the time. Both the criticism and the acknowledgment are relevant in shaping how the psychiatry field has developed.

Caption: Dr. James G. Shanklin administers electric shock and anesthesia in preparation for demonstration of a lobotomy procedure at Western State Hospital in Lakewood, Washington on July 11, 1949.
Credits: Bettmann/Contributor/Western State Hospital
By the 1950s, asylums were synonymous with poor living conditions, overcrowding, patient abuses, and general ill-treatment. Psychiatrists and staff found themselves overburdened as custodians of the mentally ill, taking in double their maximum capacity. They were also disappointed — their bet that mental illness could be ‘cured’ in these institutions didn't pan out, their ability to treat patients was nonexistent, and the perception of psychiatry was in the gutter.
Finally, deinstitutionalization
A big word to mean — in the 1950s, we decided that asylums were not the solution and that long-term psych wards should be replaced with "community mental health services".
How did this happen?
1. We fought for humane treatments.
Social-political campaigns were birthed from whistleblowers who exposed how poorly the patients were treated, questioning the necessity of a long-term institution like the asylum. This public outcry drove a lot of desire to explore alternative ways of caring for the mentally ill.
2. We discovered drugs.
The discovery of psychotropics, aka antipsychotic drugs, in the 1950s and 1960s meant that for the first time, psychotic episodes could be managed. Psychiatrists could now see a future where their patients, instead of being confined to a wall or restrained on a bed, could be safely released into a community. For a field where nothing had worked yet, this was a beacon of hope.
3. We wrote some bills and got some money.
The idea of “community mental health services” was not new — it just needed the momentum to be funded. In 1954, New York become one of the first states to reform its asylums, passing the Community Mental Health Act. This act provided funding to outpatient clinics for patients to visit for treatment (as opposed to institutions, which were the asylums). Many states did the same, moving away from asylums and towards the community services. But they all quickly encountered the same issue — who's paying?
You can thank Rosemary Kennedy because JFK came to the rescue. In 1963, President Kennedy called for reform, proposing a new approach to care for the mentally ill. Kennedy's Community Mental Health Act bill allocated $150 million in grants for the states to build these centers, with the federal government sharing up to two-thirds of the costs. These centers were required to offer 24-hour emergency services, partial hospitalization, outpatient and inpatient services, and educational work.
A little more on the Community Mental Health Act
The brainchild of just a few psychiatrists, the Community Mental Health Act (CMHA) moved the role of mental healthcare away from state institutions like the asylum, to community mental health centers. They hoped that these centers would serve as an alternative to institutionalization, allowing patients to be cared for as they worked and lived at home.
When President Kennedy signed this act in 1963, his ultimate goal was to reduce the number of patients in these institutions by 50% in 1-2 decades. It was ambitious, and few anticipated just how quickly this goal would be realized. By 1980, the number of patients had declined by 75%. By 2000, only 50,000 patients lived in state institutions, a far cry from the half a million number just 50 years prior.
This rapid decline in patient population and the closures of the state institutions were encouraged by a whole suite of policy and legislation changes, all of which moved the focus of mental health to the community. This deinstitutionalized system, where mental health care is managed by the greater “community health system”, is what continues to exist today.
The Community Health System Today
Ok, we went from madhouses to asylums, and now we have community health centers. Now what? Is this “community health” system working for us today?
As with anything healthcare in America, it gets complicated. The best answer I can give is — stay tuned for the next newsletter.
Warmly,
Vic
Thanks for sharing your inbox with me! Outside of writing this newsletter, Victoria is also the co-founder of Heard, a mental health company. If a friend forwarded you this and you like what you’re reading, please subscribe!